Article Text

Statistics from Altmetric.com
AA amyloidosis is a serious complication of chronic inflammatory and infectious diseases.1 Amyloid fibril deposition causes progressive deterioration in various organs.
In October 2007, a 50-year-old woman was admitted to our hospital with severe diarrhoea and weight loss. She had had rheumatoid arthritis (RA) for 12 years. Despite vigorous treatment with prednisolone and disease-modifying anti-rheumatic drugs (DMARDs), including bucillamine, sulfasalazine, auranofin, leflunomide and methotrexate or tacrolimus, her disease remained active.
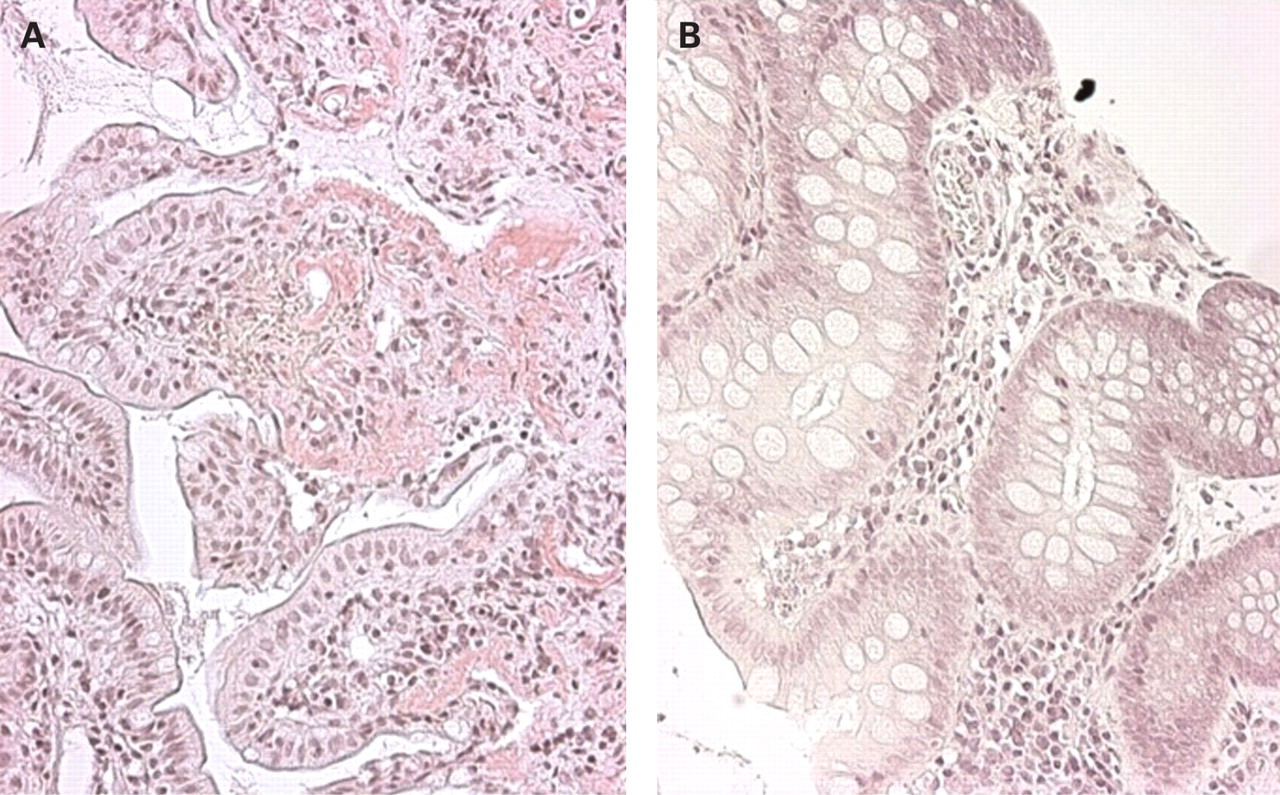
In January 2007, treatment was started with biological drugs. Subcutaneous injection of 25 mg of etanercept twice weekly for 2 months and, subsequently, intravenous injection of 3 mg/kg infliximab for 5 months combined with 20 mg of prednisolone failed to suppress disease activity as indicated by symptoms, C-reactive protein (CRP) levels of 2.4–3.9 mg/dl and serum amyloid A (SAA) levels of 13–2150 μg/ml. Colon biopsy showed marked deposits of amyloids in all three specimens from the terminal ileum and transverse colon (fig 1A). However, she had no proteinuria or renal disease. Informed consent from the patient and permission from the ethics committee of Osaka University Hospital was obtained, and administration of tocilizumab, a humanised anti-interleukin (IL) 6 receptor antibody,2 at 8 mg/kg monthly was started in November. Bowel rest combined with intravenous hyperalimentation transfusion did not improve the diarrhoea, but 2 months of tocilizumab administration stopped the diarrhoea and improved the disease activity of RA. Serum levels of CRP immediately became negative and SAA remained below 10 μg/ml. After three injections of tocilizumab, a colon biopsy was performed. No amyloid deposits were detected at two different parts of the colon (fig 1B). It was confirmed that specimens from three different parts of the colon showed no amyloid deposits 6 months after the start of tocilizumab treatment. No adverse effect was seen during the tocilizumab treatment.

{kind=link}
Amyloid A deposits were observed in the colon (A). Three months later after tocilizumab treatment amyloid A protein deposits had disappeared (B).
The recent use of anti-tumour necrosis factor (TNF) biological drugs such as infliximab and etanercept has been found to partly ameliorate organic functions and amyloid deposits in some but not all patients with AA amyloidosis,3 4 while another study reported that administration of tocilizumab showed a remarkable effect on renal function in a patient with juvenile idiopathic arthritis, reducing amyloid deposits in duodenal mucosa after 6-months’ treatment.5 Our patient had been markedly resistant to treatment with prednisolone, DMARDs and anti-TNF biological modifiers while her condition became complicated with AA amyloidosis, but promptly responded to tocilizumab; only three injections of this biological drug resulted in the disappearance of amyloid A deposits in colon. Since the activation of the SAA gene depends more on the presence of IL6 than on the presence of TNFα or IL1β,6 7 and based on the marked effect of tocilizumab reported here, tocilizumab may become a first-line treatment but additional data are needed. A randomised trial could be difficult to set up but there is clearly a need for a prospective study.
Footnotes
Funding: This study was supported by the Program for Promotion of Fundamental Studies in Health Sciences of the National Institute of Biomedical Innovation.
Competing interests: TK holds a patent for tocilizumab. The other authors declare no competing interests.
Ethics approval: Approval from the ethics committee of Osaka University Hospital.